Key points
- Rashes with fever are always worth evaluating — the combination can indicate serious conditions like meningococcemia or drug reactions.
- A rash that spreads rapidly, forms blisters across large areas, or involves mucous membranes requires urgent evaluation.
- Petechiae (pinpoint reddish-purple spots that don't blanch when pressed) can indicate a bleeding disorder or serious infection and warrant immediate attention.
- Contact dermatitis, heat rash, and viral exanthems account for the majority of adult rashes and can often be managed with OTC treatments.
- New rashes after starting a medication — especially antibiotics, anticonvulsants, or NSAIDs — should be reported to your provider promptly.
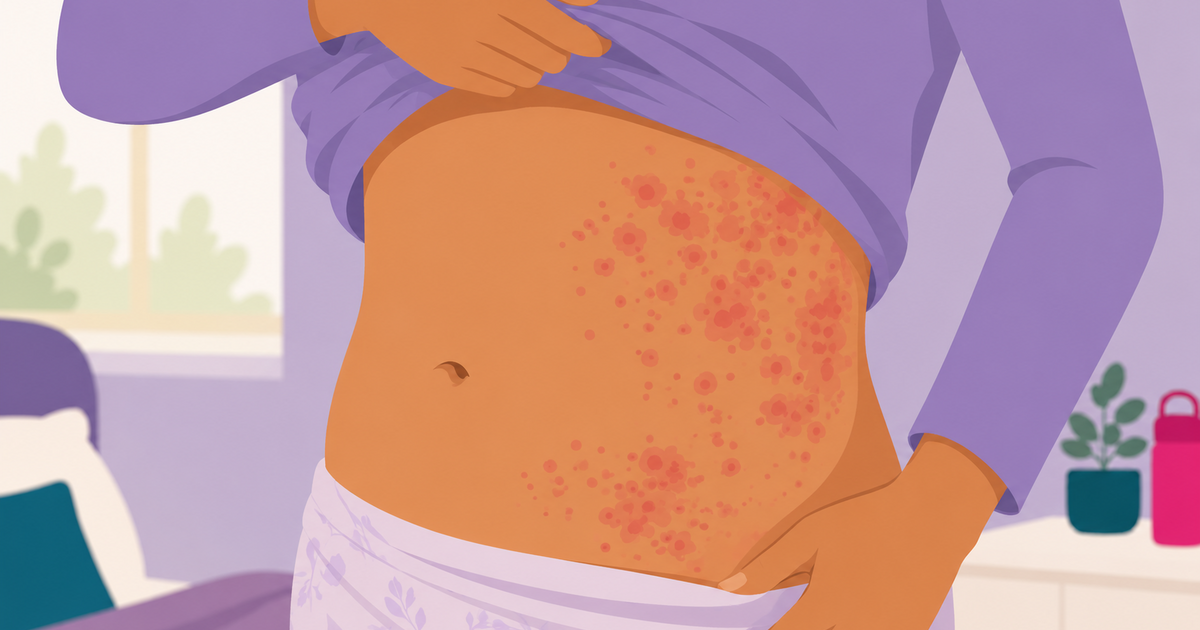
Rashes are one of the most common reasons adults seek medical care — and also one of the most anxiety-inducing. The internet's tendency to display worst-case scenarios when you search a symptom doesn't help. The reality is that most adult rashes are benign and manageable at home. But a meaningful minority signal something that warrants same-day evaluation, and a small number are genuine emergencies. This guide is designed to help you figure out which category you're in — and what to do about it.
Common rashes that usually don't need a doctor
Understanding what's common gives important context. The majority of adult rashes fall into a few well-characterized categories that are rarely serious:
Contact dermatitis is an inflammatory reaction triggered when skin contacts an irritant or allergen — poison ivy, latex, certain metals in jewelry, fragrances, or cleaning products. It typically produces itching, redness, and sometimes blistering in a pattern that mirrors the area of contact. Identifying and avoiding the trigger, combined with topical hydrocortisone cream, usually resolves the rash within 1–3 weeks.
Heat rash (miliaria) occurs when sweat ducts become blocked, causing sweat to leak into surrounding skin tissue. It produces small, itchy or prickly bumps — often in skin folds or areas covered by clothing — in hot, humid conditions. It resolves on its own once the skin cools and dries.
Viral exanthems are rashes associated with common viral illnesses. Many viruses — including certain strains of adenovirus, enterovirus, and others — produce a diffuse, flat or slightly raised red rash as part of the immune response. These typically appear as the fever breaks and resolve on their own within a few days.
Eczema (atopic dermatitis) is a chronic inflammatory skin condition that causes dry, itchy, inflamed skin. Adults with known eczema usually recognize their flares. Mild flares respond to moisturizers and OTC hydrocortisone. More severe flares may need prescription topical steroids.
Ringworm (tinea corporis) is a fungal skin infection — not an actual worm — that produces a ring-shaped, scaly, itchy rash. Over-the-counter antifungal creams like clotrimazole are usually effective when applied consistently for 2–4 weeks.
Red flags: rashes that need same-day evaluation
Certain features of a rash — or accompanying symptoms — should prompt you to seek care the same day rather than waiting to see if things improve on their own:
- Rash with fever: The combination of fever and rash narrows the differential significantly and can indicate drug hypersensitivity reactions, bacterial infections, or — rarely — serious conditions like meningococcemia. Always get evaluated.
- Petechiae: Petechiae are pinpoint reddish-purple or dark red spots caused by bleeding under the skin. The key test is the "glass test" — press a clear glass firmly against the spots. If they don't fade (blanch) under pressure, they are petechiae and not merely dilated blood vessels. Non-blanching petechiae can signal meningococcal disease, other serious bacterial infections, or blood clotting disorders. This is an urgent situation.
- Rash involving mucous membranes: A rash that affects the mouth, eyes, or genitals — especially combined with blistering — may indicate Stevens-Johnson syndrome, a rare but life-threatening drug reaction or infection. The hallmark is skin that begins to peel in sheets. This requires emergency care.
- Rapidly spreading rash with pain and fever: A rash that spreads quickly with significant pain — particularly in the context of fever — raises concern for necrotizing fasciitis or another serious soft tissue infection. The skin may look discolored, red, or swollen and may feel hard. This is an emergency.
- New rash after starting a medication: Drug-induced rashes range from benign (mild morbilliform eruptions) to life-threatening (Stevens-Johnson syndrome, drug reaction with eosinophilia and systemic symptoms — DRESS). The timing — typically 1–2 weeks after starting a new drug — is characteristic. Antibiotics, anticonvulsants, NSAIDs, and allopurinol are among the most common culprits. Notify your provider or go to urgent care promptly.
Allergic rashes and anaphylaxis
Hives — raised, irregularly shaped, intensely itchy welts that can appear anywhere on the body and change shape or location within hours — are the classic sign of an allergic skin reaction. Common triggers include foods, medications, insect stings, and latex. Hives themselves, without other symptoms, can usually be managed with oral antihistamines and monitored at home for mild cases, though persistent or recurrent hives lasting more than six weeks warrant medical evaluation to identify the underlying cause.
The urgent concern with allergic reactions is progression to anaphylaxis — a systemic, potentially life-threatening allergic response. Signs include hives combined with any of the following: swelling of the throat, lips, or tongue; difficulty breathing or swallowing; hoarseness; significant drop in blood pressure; dizziness or fainting; or vomiting. Anaphylaxis requires immediate injection of epinephrine and a call to 911. It should not be treated at urgent care unless epinephrine is immediately available and emergency backup is accessible. If you have a known severe allergy and carry an epinephrine auto-injector, use it at the first sign of a systemic reaction.
Rashes that can wait — but shouldn't be ignored indefinitely
Some rashes don't require urgent same-day care but deserve attention if they don't resolve or if additional symptoms develop. A rash that persists beyond 2–3 weeks without an obvious cause should be evaluated. Non-itchy rashes are sometimes dismissed as insignificant, but they can carry important diagnostic information. Lyme disease classically produces erythema migrans — a slowly expanding, often bull's-eye-shaped rash centered on a tick bite — that may not itch at all. Secondary syphilis produces a non-itchy rash that often involves the palms and soles. Psoriasis produces thick, silvery, scaly plaques that tend to recur. None of these are emergencies, but all warrant medical evaluation and proper diagnosis.
Shingles (herpes zoster) deserves special mention. It begins as a painful burning sensation in a dermatomal strip — typically one side of the torso or face — followed by a cluster of blisters that evolve over 7–10 days. The earlier antiviral treatment is started, the more effectively it reduces both the duration of the outbreak and the risk of post-herpetic neuralgia, a chronic pain condition. See a provider as soon as shingles is suspected — ideally within 72 hours of rash onset.
When to visit urgent care
Urgent care is an excellent resource for most rash presentations. Providers can examine the rash, take a careful history to assess for drug exposures or contact triggers, prescribe topical or systemic corticosteroids for inflammatory rashes, prescribe antifungals or antibiotics for infectious causes, and determine whether additional testing or referral is needed. If your rash has any of the red flag features described above — particularly fever, petechiae, mucous membrane involvement, or rapid spreading — go to urgent care the same day or to the ER if symptoms are severe. Solv helps you find a nearby urgent care with real-time wait times and same-day booking, so you can get a professional set of eyes on your skin without spending hours in a waiting room.
Frequently asked questions
What does a dangerous rash look like?
Red flags include: rash with fever; petechiae (non-blanching red/purple dots); rash involving mouth, eyes, or genitals; blistering across large areas; rapidly spreading redness; or rash after starting a new medication.
How do I tell if a rash is an allergic reaction?
Allergic rashes (hives) appear as raised, itchy welts that can appear and disappear quickly. If accompanied by throat tightness, difficulty breathing, lip or tongue swelling, or dizziness — that's anaphylaxis. Call 911 immediately.
Can urgent care treat a rash?
Yes. Urgent care can diagnose and treat most common rash presentations including allergic reactions, contact dermatitis, cellulitis, ringworm, eczema flares, and viral rashes.
What causes a rash that doesn't itch?
Non-itchy rashes can be caused by viral infections, drug reactions, vasculitis, or Lyme disease (target-shaped erythema migrans). A non-itchy rash that persists or comes with other symptoms deserves evaluation.
Should I go to urgent care or the ER for a rash?
Most rashes can be evaluated at urgent care. Go to the ER if the rash is accompanied by difficulty breathing, throat swelling, severe facial swelling, confusion, rapidly spreading painful rash with fever, or petechiae.

Dr. Linda Halbrook is a Board-Certified Family Medicine physician with over 40 years of experience, dedicated to providing comprehensive care to patients across Texas. She retired from practice but currently serves on the Clinical Services Committee of CommonGood Medical, a non-profit organization serving the uninsured in Collin County.
How we reviewed this article
Medically reviewed
View this article's sources and history, and read more about Solv's Content Mission Statement, editorial process, and editorial team.
6 sources
Solv has strict sourcing guidelines and relies on peer-reviewed studies, academic research institutions, and medical associations. We avoid using tertiary references.
- Rashes. (November 15, 2022)
- Chang WC, et al.. SJS/TEN 2019: From science to translation. J Dermatol Sci. (2020)
- Meningococcal disease: clinical information. (January 19, 2023)
- Lyme disease: signs and symptoms. (January 19, 2023)
- Drug-induced skin reactions. (September 15, 2010)
- Anaphylaxis. (October 15, 2023)
Solv’s team of medical writers and experts review and update our articles when new information becomes available.
May 20 2026
Written by Solv Editorial Team
Medically reviewed by: Dr. Rob Rohatsch, MD
May 01 2026
Edited by Solv Editorial Team
May 21 2026
Edited by Solv Editorial Team
May 22 2026
Edited by Solv Editorial Team
May 26 2026
Edited by Solv Editorial Team
June 03 2026
Edited by Solv Editorial Team